Abstract
A review of prerequisites for vacuum extraction: Appropriate position of the fetal head for vacuum extraction from a forceps delivery perspective
As the frequency of forceps delivery has lowered in recent years, the use of vacuum extraction has become the technique of choice for forced delivery due to its technical ease and low risk for maternal injury. However, the success rate of vaginal births by vacuum extraction is lower than for forceps delivery and the risk for fetal injury is higher, which has led to an overall increase in legal cases concerning vacuum extraction. Prerequisites for vacuum extraction are based on those for forceps delivery according to the American College of Obstetricians and Gynecologists (ACOG) guidelines, wherein delivery is performed for fetal head positions at station +0 or lower. In Japan, forceps delivery is contraindicated when the fetal head is higher than at station +2, while in the United States (US), mid forceps delivery, defined by a fetal head position higher than station +2, is only occasionally performed due to the technical difficulty of the method. Forceps delivery is usually indicated for a fetal head position at station +2 or lower, with an injury rate that is lower than for vacuum extraction. Consequently, as vacuum extraction has a weaker pulling power than forceps, it is a theoretical contradiction that vacuum extraction is being performed at fetal head heights for which forceps delivery is not recommended. Therefore, we propose that vacuum extraction ought to be performed only in cases in which the fetal head height is at least at station +2 or lower to improve the success rate of vaginal births and reduce the complications to mother and fetus from vacuum extraction.
Author(s):
Hiroyuki Sekia and Satoru Takedab
Abstract | Full-Text | PDF
Share this

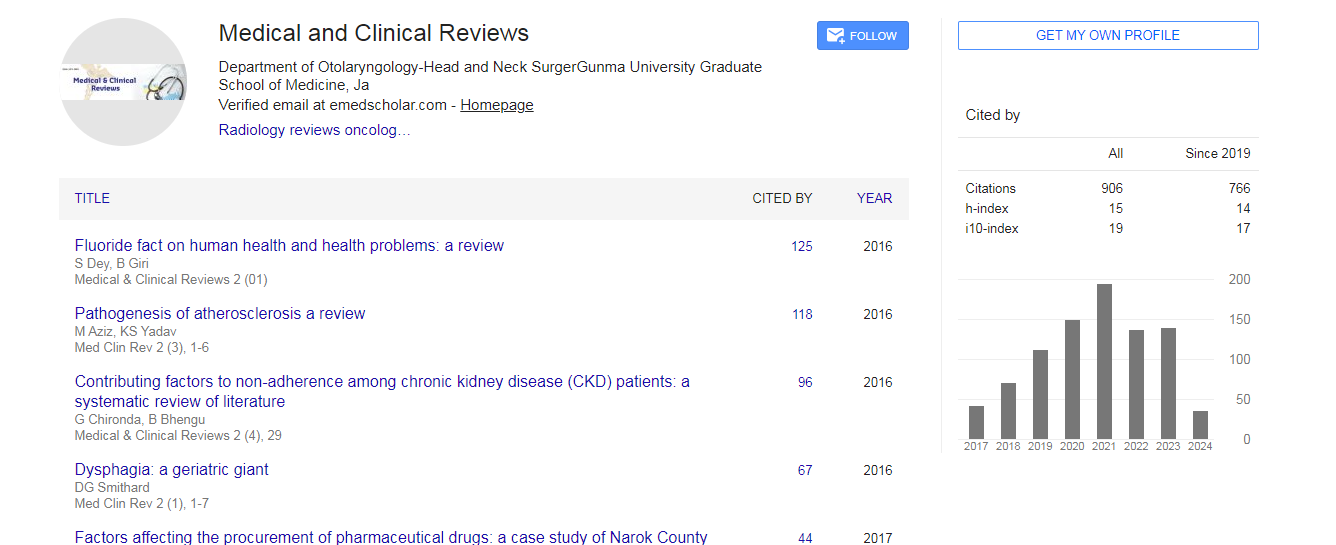
Google scholar citation report
Citations : 906
Medical & Clinical Reviews received 906 citations as per google scholar report
Medical & Clinical Reviews peer review process verified at publons
Abstracted/Indexed in
- Google Scholar
- China National Knowledge Infrastructure (CNKI)
- Directory of Research Journal Indexing (DRJI)
- WorldCat
- Publons
- Secret Search Engine Labs


Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences